KEMIRIX
Clinical AI that catches dangerous drug prescriptions before they reach the patient
KEMIRIX checks every drug combination against the patient's full picture — kidney function, genetics, and traditional medicine use — all at once, in real time. Every answer is backed by real clinical evidence. Not guesswork.
Why we are building this
Every day, preventable medication errors cause serious harm in African hospitals.
Prescribers are working without a safety net. Drug combinations go unchecked. A patient's failing kidneys change how a drug behaves — but nobody flags it. Patients use traditional herbs alongside their prescriptions, and most clinical software doesn't even know to look.
These aren't rare edge cases. They're everyday situations in Kenyan hospitals, Nigerian clinics, and across East Africa — and they lead to real harm.
KEMIRIX was built specifically for this environment. For the pharmacists, doctors, and nurses who need a reliable second opinion before a dangerous prescription reaches a patient.
How it works
Three steps. One clear answer.
Enter the patient's prescriptions
A doctor, pharmacist, or nurse enters the patient's current medications, lab results like kidney function, and any traditional remedies they're taking.
KEMIRIX runs a full safety check
The engine checks for dangerous drug combinations, organ function risks, genetic factors that affect how a drug is processed, and interactions with African traditional medicine — all in real time.
The clinician gets a clear, actionable report
No medical jargon overload. A plain recommendation: what to stop, what to change, what to monitor — with the clinical evidence behind every decision.
Built For Every Role
BUILT FOR EVERY ROLE IN HEALTHCARE
One platform. Six clinical perspectives. One mission.
Doctors / Physicians
Specialist-grade reasoning. Always on.
- Differential diagnosis support with citation trails
- Drug interaction alerts across 4 medicine systems
- Pharmacogenomics flags before prescribing
- Lab trend analysis and missed abnormal value detection
How KEMIRIX Helps
KEMIRIX becomes your clinical co-pilot — not replacing your judgment, but ensuring you never miss a dangerous interaction, a missed abnormal, or a pharmacogenomic risk that your patient carries.
How you access KEMIRIX
A subscription platform — for individuals and institutions
KEMIRIX is a SaaS platform. You subscribe, you get access. No hardware, no installation — works in the browser.
Individual clinicians
For doctors, pharmacists, and nurses who want medication safety checks at their fingertips — wherever they work.
Hospitals & clinics
Institution-wide access for your entire clinical team — one plan, every department, every prescriber covered.
Pricing will be published at launch. Early access partners receive preferential rates.
Request Early AccessHow it works in practice
A walkthrough of a real clinical case
Warfarin + Aspirin. A dangerous combination. Here is exactly what KEMIRIX does when a clinician enters it.
KEMIRIX checks across four dimensions at once
The moment a prescription is entered, KEMIRIX runs it through four layers simultaneously — drug interactions, organ function, the patient's genetics, and any traditional medicine they're taking. Most systems check one. KEMIRIX checks all four.
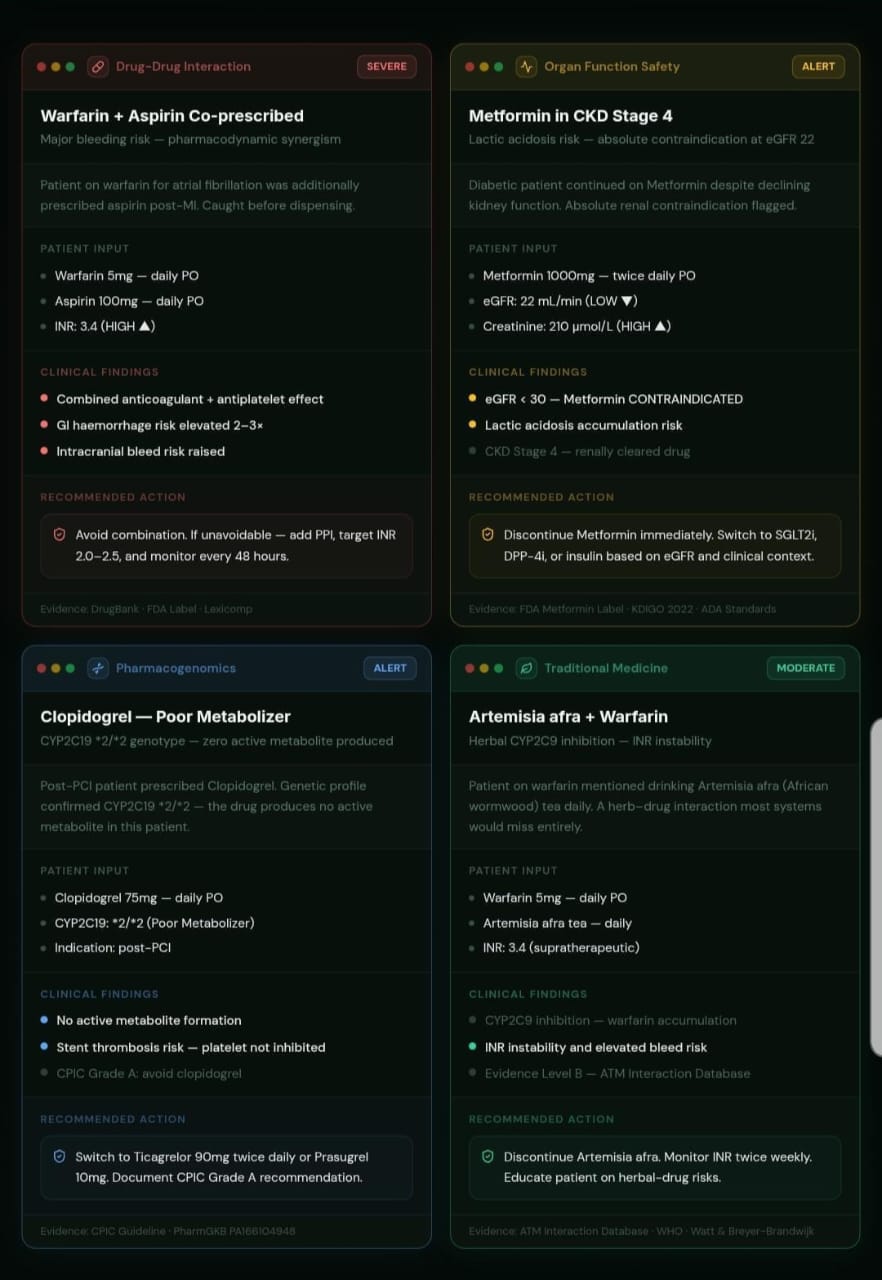
Every case is broken down clearly
Each risk is presented plainly — what the patient is taking, what KEMIRIX found, and exactly what to do next. No jargon. No ambiguity. Just a clear clinical picture with the evidence behind it.
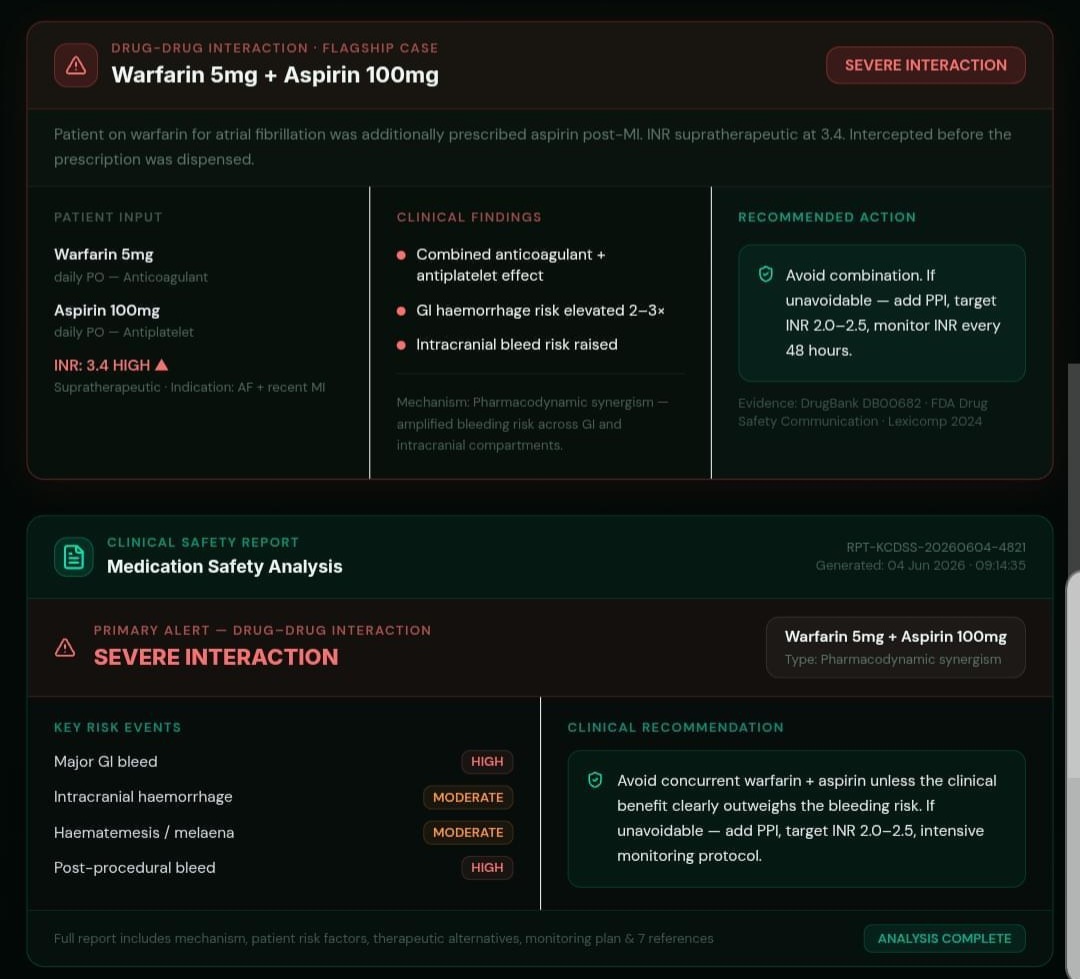
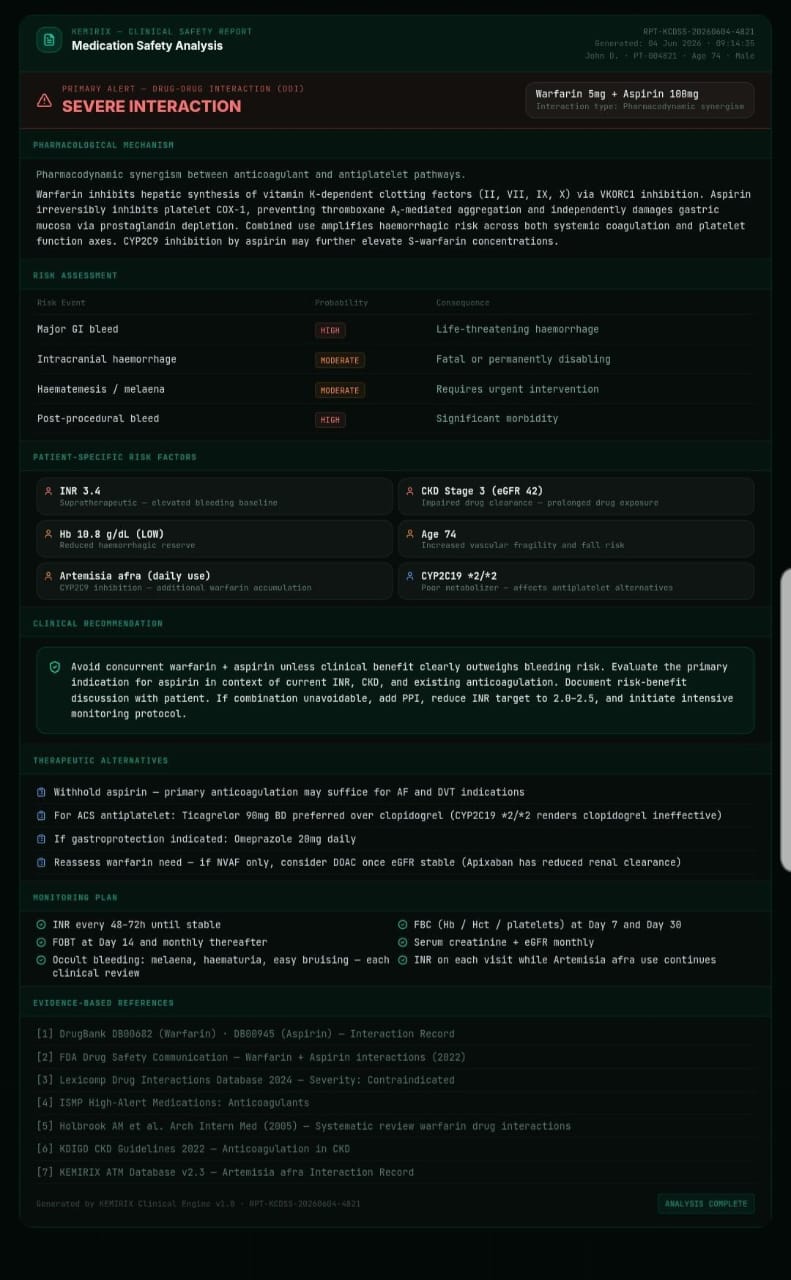
A full clinical report — referenced and actionable
Every analysis generates a complete Medication Safety Report. Pharmacological mechanism, risk assessment, patient-specific factors, therapeutic alternatives, a monitoring plan, and the clinical references behind every decision. One report. Everything a clinician needs.
Where we are today
We're building KEMIRIX. The clinical AI engine is working. We're now in the production phase — training, evaluating, and preparing for clinical validation with advisors in Kenya.
Built & Working Now
- Clinical medication safety analysis engine
- Drug-Drug Interaction detection — 4 medicine systems
- Renal & hepatic function-based dosing alerts
- Pharmacogenomics engine — African population variants
- African Traditional Medicine interaction screening
- Evidence-based recommendations (DrugBank, CPIC, FDA)
- Contraindication detection across full medication list
- Clinical report generation with monitoring protocols
- Interactive sandbox demo — 5 live clinical cases
Development Roadmap
Current Focus
Clinical AI Engine — Phase 1
Building and validating the clinical safety analysis engine with clinical advisors in Kenya and India.
Q4 2026
Alpha testing with clinical advisors — Kenya & India
Q1 2027
First hospital pilot launch — East Africa
2027
Pan-African expansion — 10+ countries
2028
Global emerging markets rollout
Regulatory Compliance & Licensing
The Team
The people building this
A small team with a clear purpose — medicine, engineering, and a deep understanding of African healthcare.

Emmanuel Bain
Co-Founder & CPO
AI/ML Engineer and Pharmacy specialist who designed and built the KEMIRIX clinical AI engine from the ground up. He built it because he understood the problem from both sides — the pharmacy and the engineering.

Abu Bakr Dahir Hassan
Co-Founder & CTO
Responsible for developing the training pipeline, model architecture, and the full-stack infrastructure of the KEMIRIX platform.
Siham Deq Hassan
Co-Founder & CEO
Medical Student driving KEMIRIX's clinical validation strategy, ensuring every feature is grounded in real-world medical accuracy and clinical workflow.
Stay in the loop
We send updates when things actually happen — new features, pilot launches, and lessons from building clinical AI for Africa.
No spam. Unsubscribe anytime.
Want to bring KEMIRIX to your hospital or clinic?
✦ Bismillahi Rhamani Rhaheem · Africa First. World Next.